Learning Center: Access information in greater detail.
Gastric feeding tube (G tube) placement considerations
When the swallowing mechanism is ineffective or unsafe, but the digestive tract from the stomach onwards is working, a feeding tube allows nutrition, fluids, and medicines to be delivered to the gut. Whether and when to undergo placement of a feeding tube, and which type (gastrostomy tube or nasogastric tube) is a decision based on several factors.
A gastric feeding tube may be recommended when someone is unable to eat or drink enough by mouth to meet their body's nutritional needs. This can happen for many reasons — for example, difficulty swallowing due to a stroke or neurological condition, blockages or injuries in the throat or esophagus, or prolonged illness that leaves a person too weak or too drowsy to eat safely. In the setting of head and neck cancer, treatments may be expected to interrupt swallowing for a period during and after treatments.
Two common types of stomach feeding tubes:
Nasogastric (NG) Tube
A thin, flexible tube inserted through your nose, down your throat, and into your stomach.
It does not require surgery — it can be placed at the bedside.
It is typically used for short-term feeding (days to a few weeks).
It can cause some discomfort in the nose and throat and may occasionally shift out of place.
Gastrostomy (G) Tube
A tube placed directly through the skin of your abdomen into your stomach.
It requires a minor procedure to place, usually done with a camera (endoscope) or with imaging guidance.
It is used for long-term feeding (weeks, months, or longer).
Because it doesn't go through your nose or throat, it is generally more comfortable for extended use and less visible under clothing.
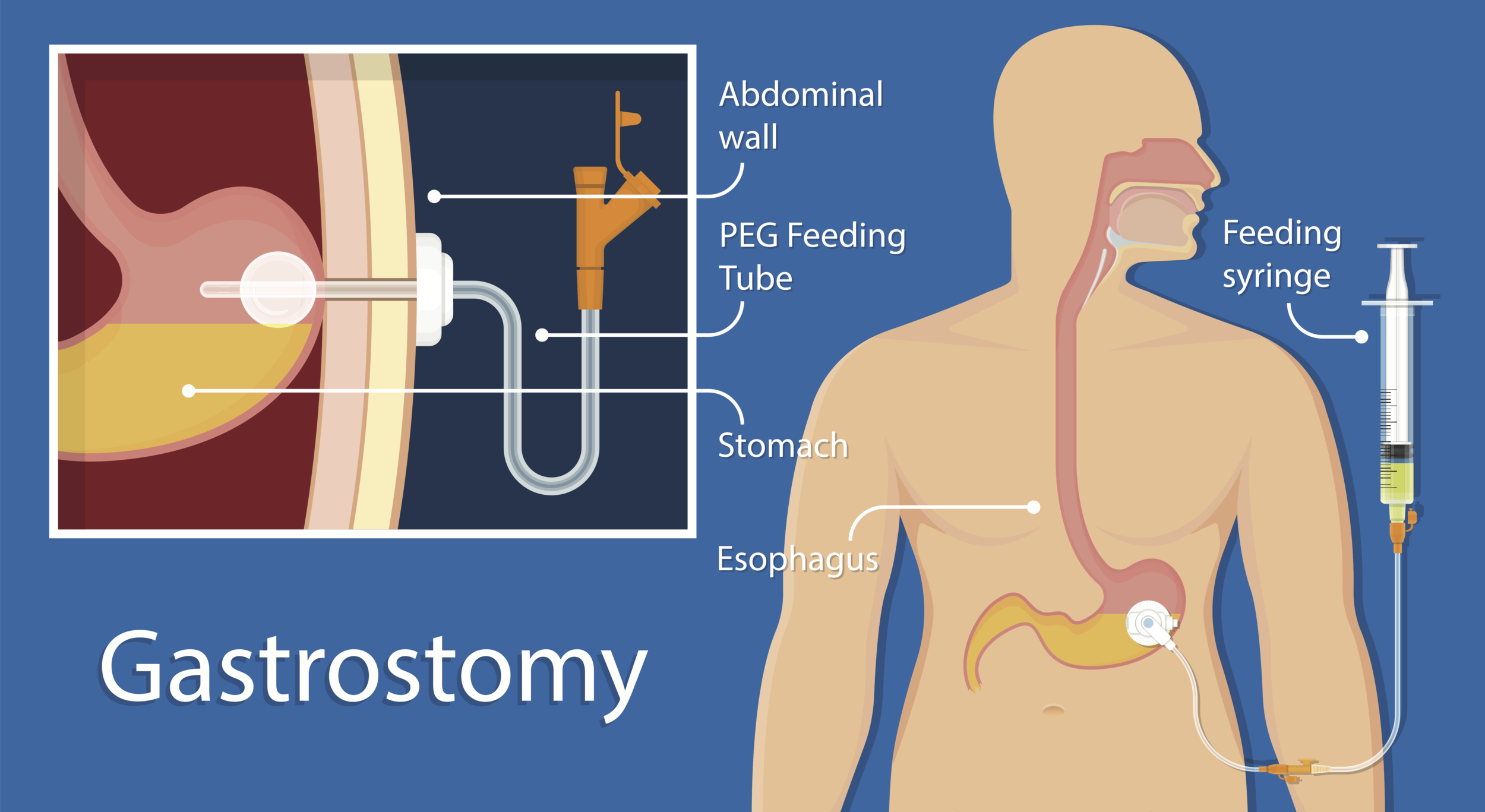
A gastrostomy feeding tube (G-tube) is a tube that passes through the skin of the abdomen directly to the stomach.
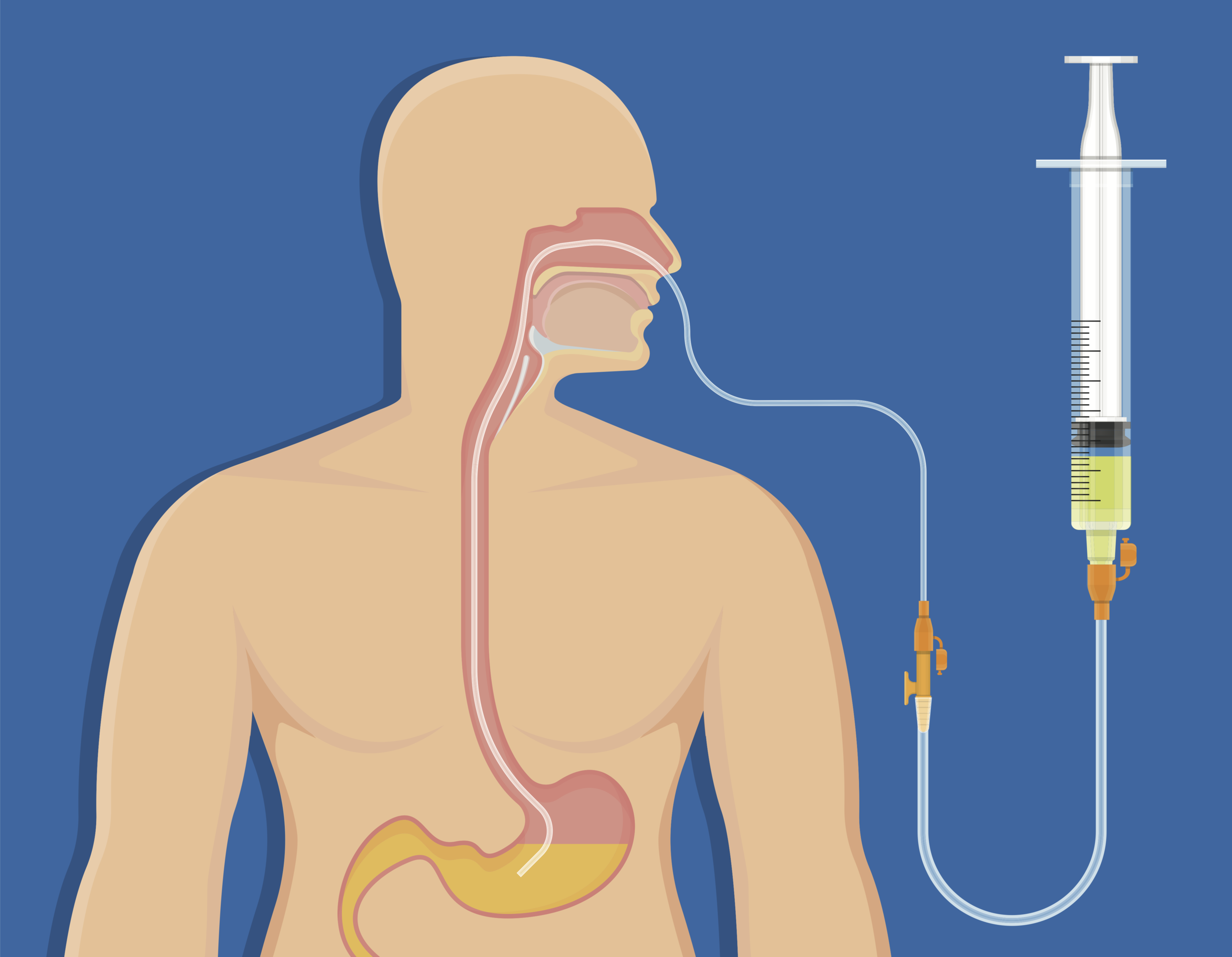
A nasogastric feeding tube (NG tube) is a tube that passes through the nose, down the throat and esophagus to the stomach.
ADVANTAGES OF A Gastrostomy TUBE (through the abdominal wall)
When tube feeding is needed for more than a few weeks, a gastrostomy tube (a tube placed directly through the skin into the stomach) offers several advantages over a nasogastric tube (a tube that goes through the nose and down the throat):
More Comfortable
Because the tube does not pass through your nose and throat, a gastrostomy tube is generally much more comfortable for daily life. There is no constant irritation in your nose or throat, and it does not interfere with breathing, talking, or swallowing.
Easier to Live With
A gastrostomy tube sits flat against your abdomen and can be hidden under clothing. This makes it less noticeable and easier to manage at home, at work, or in social settings compared to a tube taped to your face.
Less Likely to Come Out of Place
Nasogastric tubes can accidentally slip out or shift position, which may require reinsertion. A gastrostomy tube is held securely in place and is much less likely to move.
Fewer Complications Over Time
Long-term use of a nasogastric tube can cause irritation or sores in the nose, throat, and esophagus, and may increase the risk of sinus infections. A gastrostomy tube avoids these problems.
Easier to Feed Through
Gastrostomy tubes are often wider, which means feedings and medications can flow through more easily and the tube is less likely to clog.
Suitable for Outpatient Use
After the first 24-72 hours from placement, gastrostomy tubes are considered safe for use as an outpatient, often with some skilled assistance such as through home health at least until the individual develops skill and comfort performing feedings and tube care.
DISADVANTAGES OF A G TUBE (through the abdominal wall)
While a gastrostomy tube has many benefits for long-term feeding, there are some disadvantages compared to a nasogastric tube that are important to understand:
Requires a Medical Procedure
A gastrostomy tube must be placed during a procedure — usually using a small camera (endoscope) passed through the mouth while you are sedated. A nasogastric tube, by contrast, can be placed quickly at the bedside without sedation or a procedure room.
Higher Upfront Cost
Because gastrostomy tube placement involves a procedure, specialized equipment, and a medical team, it costs significantly more to place than a nasogastric tube.
Risks Related to the Procedure
Although gastrostomy placement is generally safe, any procedure carries some risk. Possible complications include:
Infection at the tube site on the abdomen (the most common complication)
Pain or soreness at the site after placement
Minor bleeding
Rarely, more serious problems such as injury to nearby organs or leakage into the abdominal cavity
Ongoing Site Care
The skin around the gastrostomy tube needs regular cleaning and monitoring to prevent infection, irritation, or leakage. A nasogastric tube does not require this type of wound care.
Tube-Related Problems Over Time
Over weeks or months, a gastrostomy tube can develop issues such as:
The tube becoming clogged or breaking down
Leakage of stomach contents around the tube site
The internal part of the tube migrating into the stomach wall (called "buried bumper syndrome")
Accidental removal, which may require urgent medical attention — especially in the first few weeks before the opening has fully healed
Not Suitable for Everyone
Some medical conditions may prevent safe placement of a gastrostomy tube, including severe fluid buildup in the abdomen (ascites), certain blood clotting problems, or abdominal infections.
Important to Remember
Despite these disadvantages, a gastrostomy tube is still considered the better option when tube feeding is needed for more than about four weeks.
Advantages of a nasogastric feeding tube
When tube feeding is only needed for a short time, a nasogastric tube (a thin, flexible tube passed through the nose and down into the stomach) has several advantages over a gastrostomy tube (a tube placed through the skin into the stomach):
No Procedure or Surgery Needed
A nasogastric tube can be placed quickly and easily at the bedside by a nurse or doctor. There is no need for sedation, an operating room, or special equipment. This means it can be started right away when feeding is needed urgently.
Lower Risk
Because no incision or procedure is involved, a nasogastric tube avoids the risks that come with gastrostomy placement, such as infection at a wound site, bleeding, or injury to internal organs.
Easily Removed
When you no longer need tube feeding, a nasogastric tube can be gently pulled out in seconds at the bedside. There is no wound left behind and no healing time needed. A gastrostomy tube, by contrast, leaves a small opening in the abdomen that takes time to close after removal.
Lower Cost
A nasogastric tube is far less expensive to place than a gastrostomy tube, since it does not require a procedure, sedation, or a specialist.
No Wound to Care For
With a nasogastric tube, there is no opening in the skin that needs daily cleaning or monitoring. This means less daily maintenance and no risk of skin irritation or infection around a tube site on the abdomen.
Good Option While Decisions Are Being Made
A nasogastric tube is an excellent temporary solution while your medical team determines whether you will recover the ability to eat on your own or whether a longer-term feeding tube is needed. It allows nutrition to be started quickly without committing to a more permanent option.
Important to Remember
A nasogastric tube works best for short-term use — generally up to about four weeks.
Disadvantages of a nasogastric feeding tube
While a nasogastric tube (a tube passed through the nose into the stomach) is a good short-term option, it has several disadvantages compared to a gastrostomy tube (a tube placed directly through the skin into the stomach), especially as time goes on:
Less Comfortable
The tube sits in your nose and runs down the back of your throat at all times. This can cause a constant feeling of irritation, gagging, or soreness in the nose and throat. Many patients find it difficult to get used to.
More Visible and Harder to Live With
A nasogastric tube is taped to the face and clearly visible to others. This can feel embarrassing or distressing, particularly in social situations. A gastrostomy tube, by contrast, is hidden under clothing on the abdomen.
Can Easily Come Out or Shift Position
Nasogastric tubes can be accidentally pulled out — for example, during sleep, coughing, or confusion. When this happens, the tube must be reinserted, which can be uncomfortable. If the tube shifts out of position without being noticed, feeding could go to the wrong place, which can be dangerous.
Irritation and Injury Over Time
Prolonged use of a nasogastric tube can lead to:
Sores or ulcers inside the nose
Irritation or damage to the throat and esophagus (the swallowing tube)
Sinus infections from blockage of the normal drainage pathways
Ear discomfort
These problems become more likely the longer the tube stays in place.
Higher Risk of Aspiration
A nasogastric tube may interfere with the normal closing of the valve between the esophagus and stomach, which can increase the chance of stomach contents flowing back up into the throat and lungs. This is called aspiration and can lead to pneumonia.
Interferes With Swallowing and Speaking
The tube running through the throat can make it harder to swallow your own saliva or practice eating, and may affect your voice. This can slow down rehabilitation for patients who are working to regain the ability to eat.
More Likely to Clog
Nasogastric tubes are generally narrower than gastrostomy tubes, which means they are more prone to clogging — especially with thicker feeds or crushed medications.
Not Ideal for Long-Term or Outpatient Use
A nasogastric tube is designed as a temporary solution, generally for up to about four weeks. If feeding is needed beyond that time, the ongoing discomfort, complications, and inconvenience make it a poor choice compared to a gastrostomy tube. A nasogastric tube is typically not suitable for use outside of a hospital or health facility setting because of safety concerns related to the tube slipping partially out and leading to aspiration pneumonia.
When and whether to use a feeding tube: my usual recommendations for head and neck cancer patients
Each situation is individual and my advice is tailored to a patient’s situation. Young, motivated, otherwise healthy and robust patients in general have a better chance of gleaning the benefit of maintaining swallowing function without compromising nutrition or risking lung infection without a feeding tube, whereas the already malnourished patient who has bad lungs or swallowing already compromised by the tumor may be best served by having a gastrostomy tube placed early in the treatment process.
Removal of a Feeding tube
Generally, removal of a gastrostomy tube may be undertaken when it is highly likely the patient no longer needs it. In my practice, when swallowing has improved since placement of the feeding tube and it appears as if the gastric feeding tube may no longer be necessary, I usually like to see a patient maintain or gain weight with an oral diet (not using the G tube at all) for one month, before I think it is safe for G tube removal. The risk of removing the G tube before someone can sustain adequate intake by mouth is that weight loss and dehydration may occur, and the G tube may need to be replaced in a repeat procedure. Removal of a G tube is typically undertaken by the physician who placed it originally, or one of their partners, who will also provide wound care instructions.
Removal of a nasogastric tube is simpler undertaking. Any retaining stitch or tape holding the tube in place is removed and the tube may be pulled out. Because of the simplicity of removing a nasogastric tube as well as the relative simplicity of replacing it, if necessary, criteria to meet before removing a nasogastric tube are usually less stringent than with a G tube.
Learning Center Main Index:
Throat:
swallowing, tonsils and adenoids, obstructive sleep apnea, voice
Aesthetics:
skin regimen, injectables {neuromodulators (e,g. Botox), hyaluronic acid fillers (e.g., Juvederm), and others}, rhinoplasty, facelift, neck lift, and brow lift, blepharoplasty (eyelid surgery), skin resurfacing, scar treatment
Tumors (benign and malignant/cancerous):
general tumor information, thyroid, parathyroid, skin, neck, oropharynx, larynx (voice box), salivary gland, nose and sinus, oral cavity (mouth and lips), nasopharynx, hypopharynx, radiation therapy, chemotherapy and immunotherapy, gastric feeding tube
Nose and Sinus:
rhinoplasty (functional and cosmetic), sinusitis, breathing