Treatments: Hyperparathyroidism
Hyperparathyroidism is a condition in which too much parathyroid hormone is produced. This occurs when one or more parathyroid glands loses its ability to reduce parathyroid hormone production when it is appropriate to do so.
parathyroidectomy

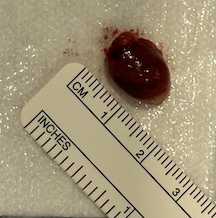
Parathyroid adenoma. This parathyroid gland is about 20 times the size (by volume) of a normal parathyroid gland. Click to enlarge the photo.
Surgical removal of one or more parathyroid glands (parathyroidectomy) remains the mainstay for treatment of primary hyperparathyroidism as it renders a cure about 95% of cases. Surgery is indicated for selected cases of tertiary hyperparathyroidism, but rarely for secondary hyperparathyroidism when medications prove ineffective. Among cases of primary hyperparathyroidism, 85% are caused by a single overactive parathyroid gland, and its removal yields cure. Fortunately, due to two relatively recent advances (parathyroid imaging studies and intraoperative PTH measurements), parathyroidectomy may be performed in a minimally invasive approach with very high success rate. Pre-operative localization of the overactive parathyroid(s) may be done several ways, including use of a sestamibi or a SPECT scan.

Medical treatment of hyperparathyroidism
Medical treatment of hyperparathyroidism is used in the following situations:
• Secondary hyperparathyroidism, which is caused by kidney disease
• Primary hyperparathyroidism in certain exceptional scenarios:
• when the affected individual is not healthy enough to undergo parathyroid surgery
• mild primary hyperparathyroidism when surgery needs to be delayed
A group of drugs known as calcimimetics has been approved by the Food and Drug Administration for the treatment of secondary hyperparathyroidism (which is caused by kidney disease). Drugs in this category include cinacalcet (Sensipar®) to be taken by mouth, and the injectable medication etelcalcetide (Parsabiv®). These drugs cause lowering of parathyroid hormone (PTH) levels by increasing the sensitivity of the calcium-sensing receptor (CaSR) in parathyroid cells. Although calcimimetics are intended for secondary hyperparathyroidism, some physicians prescribe them selectively for primary hyperparathyroidism.
Alternatively, possibly to put surgery off while one is healing from another medical problem, mild hyperparathyroidism could be managed with plenty of hydration, possibly a calcium wasting diuretic (“water pill”) that lowers blood calcium, and avoidance of drugs like lithium or thiazide diuretics that increase blood calcium. If this route is taken, then monitoring blood calcium levels (every 6 months), blood pressure (every 6 months), kidney function (every year), and bone density (every 1 to 3 years) is typically performed by the primary care physician.
What are the reasons/indications for undertaking parathyroidectomy?

Primary Hyperparathyroidism: This is the most common indication, where surgery is often recommended for patients with:
High serum calcium levels (>1 mg/dL above the normal range).
Symptoms of hypercalcemia (e.g., kidney stones, osteoporosis, fractures, fatigue, or gastrointestinal symptoms).
Bone disease associated with hyperparathyroidism.
The incidence of a single parathyroid adenoma is significantly more common in primary hyperparathyroidism compared to the rarer occurrences of double adenomas or four-gland hyperplasia.
Parathyroid Cancer: Parathyroid cancer is very rare, accounting for 1% of cases of primary hyperparathyroidism. Surgical intervention is required for the removal of malignant parathyroid tumors, primarily because of the risks associated with extreme elevation in blood calcium, but also because of the additional risks of cancer, such as invasion into normal structures, such as the recurrent laryngeal nerve, which controls the vocal cord.
Secondary Hyperparathyroidism: In cases where the hyperparathyroidism is caused by chronic kidney disease and results in severe symptoms that do not respond to medical management.
Tertiary Hyperparathyroidism: This occurs when parathyroid glands become autonomously functioning after long-standing secondary hyperparathyroidism after the kidney disease is cured (with a kidney transplant).

parathyroid autotransplantation into the neck
During surgery of or near the parathyroid glands (such as thyroid surgery, neck dissection, or laryngectomy), one or more parathyroid glands may be found to have lost their blood supply during the dissection. If there is no reason to believe a parathyroid in this situation is diseased (such as with four gland parathyroid hyperplasia), it may be reimplanted into a readily available neck muscle (such as the sternocleidomastoid muscle). This half of a gland may take up to a month to begin functioning again, but it usually does and then maintains normal parathyroid and calcium status

parathyroid autotransplantation into the forearm
On occasion, when all parathyroid glands are overactive, surgery is undertaken whereby all glands are removed, but one half of one gland is re-implanted into a muscle away from the neck. When all parathyroid glands are overactive, this half parathyroid gland can eventually hypertrophy and lead to a recurrence of hyperparathyroidism. Alternatively, recurrence of hyperparathyroidism after thyroid surgery could indicate that an overactive gland in the neck was not identified and removed during previous surgery. A missed parathyroid gland could be the result of the notorious variability in parathyroid glands, not only in their location but also their number as some people have fewer or greater than four parathyroids. Use of the forearm as a recipient site for a transplanted parathyroid is done to prepare for future contingencies. For example, if initial parathyroid surgery yields a cure that then over time gives way to recurrent hyperparathyroidism, one would need to know if there is still hyperfunctioning parathyroid in the neck versus possible over-growth of the implanted half-gland in the arm. Two simultaneous blood draws from the left and right upper arm would indicate whether the overactivity is from the implanted arm or not. If the PTH level is significantly higher in the implanted arm than the other arm, then a relatively safer procedure may be performed to reduce the size of the implanted parathyroid gland may be undertaken. If, on the other hand, the parathyroid hormone level is equal in both arms, then chances are good that a retained parathyroid gland in the neck or chest exists, and a localizing study may be used to help locate it prior to surgery. If the overactive gland is found to be where a half gland had been implanted in the forearm, a safe and simple procedure removing some of this parathyroid gland from the arm may be done, avoiding risk to the laryngeal nerves that would be surrounded by scar tissue from the original neck surgery.

managing post-operative hypoparathyroidism (abnormally low parathyroid hormone levels)
Just as with muscles lose strength and volume when unused, parathyroids that are not active will also atrophy—shrinking and losing ability to produce parathyroid hormone. When one parathyroid is over-active, thus raising the calcium level in the blood, the other parathyroid glands appropriately reduce their own production of parathyroid hormone, becoming inactive. Once surgery is undertaken and the overactive gland (or glands) has been removed, the other glands do have the ability to build up and produce the needed amount of parathyroid hormone, but this typically takes weeks. This is typically treated with oral calcium carbonate (such as Tums), and sometimes also with progressively more potent medications, such as vitamin D, calcium administer intravenously (while in the hospital), and even synthetic (recombinant) parathyroid hormone (Natpara®). Low blood calcium can be identified with a blood test, and can be associated with symptoms such as a tingling or numbness sensation in the fingertips or lips. Very low calcium levels can also cause muscle spasms, seizures, or irregularities in the heart rhythm. Long term low calcium can lead to (or accelerate) development of weak bones (osteopenia or the more severe form, osteoporosis).

This page