Treatments: Eustachian Tube Dysfunction
Normally, the air pressure on each side of the eardrum is equal. When the Eustachian tube is dysfunctional, a difference in the air pressures arises, causing a range of problems. Treatments for Eustachian tube dysfunction include minimizing inflammation of the Eustachian tube opening, widening (dilating) the Eustachian tube, and creating of a small ventilation hole in the eardrum.
See also:
Treatment of eustachian tube dysfunction

First line treatment for Eustachian tube dysfunction is directed at treating the underlying cause through non-invasive efforts. The discussion below will detail management of the Eustachian tube that is closed too much. The less common problem of the Eustachian tube being open too much—called a patulous Eustachian tube—is discussed separately.
Non-surgical management of Eustachian tube dysfunction:

In essence, mainstay goal for relieving obstruction of the Eustachian tube that does not open adequately is to make the passageway larger. Since swelling of soft tissue surface lining, particularly at the opening of the Eustachian tube, located in the throat, is the typical cause of Eustachian tube dysfunction, decreasing this swelling may be accomplished through a variety of actions:
Treat associated infection, if present. This may be infection of the sinuses, tonsils, and or adenoids. Viral infections are managed with time and general supportive measures, whereas bacterial infections may require antibiotics.
Treat associated reflux. In adults, reflux of stomach contents is a common cause of Eustachian tube dysfunction. This fact may be surprising until one understands that reflux of stomach acid and digestive enzymes often passes upward through the esophagus to reach the throat, where the Eustachian tube orifice is located. Treatment for reflux may prove helpful for Eustachian tube dysfunction.
Opening the Eustachian tube. Understanding normal Eustachian tube function facilitates understanding of why swallowing or yawning is a quick and simple treatment options for Eustachian tube dysfunction. When swallowing or yawning, a muscle (the tensor veli palatine muscle) pulls on the Eustachian tube orifice in a direction that helps to open the passageway. Therefore, encouraging swallowing by drinking fluids, chewing gum, or having a hard candy may help.
Push air up the Eustachian tube. Separate from enlarging the Eustachian tube passageway by muscle activation is auto-insufflation, also known as “popping” ones ears. This is a technique in which a person increases the air pressure in the throat, thus using gentle force to push air up through the Eustachian tube to the middle ear. To voluntarily “pop” the ears, one pinches the nostrils closed while otherwise simulating blowing one’s nose. In doing so, the increased air pressure in the throat facilitates moving air up the Eustachian tube to the ear.
Use of a nasal decongestant spray. Medicines like oxymetazoline (Afrin) and phenylephrine (Neo-synephrine, Sinex) may be sprayed in the nose and absorbed from the mucosal surface lining to constrict blood vessels and markedly shrink the soft tissue. The effect is strong, but after about 12 hours, rebound swelling may set in. Repeated use of a topical nasal decongestant for more than 3 days can lead to a major problem of nasal decongestant addiction called rhinitis medicamentosa. Use of nasal decongestant sprays must be limited to fewer than 3 days per month.
Use of a systemic decongestant. A decongestant taken in pill form is absorbed into the bloodstream, which circulates the medicine throughout the body, including the Eustachian tube opening but also the brain, heart and blood vessels, eyes and bladder. Side effects of this medication’s effect on those non-target organs include headache, insomnia, anxiety, irritability, fast or irregular heart beats, increase pressure in the eye, and worsening of urinary blockage, especially in men.
Use of a nasal steroid spray. Steroids reduce inflammation. Spraying a steroid medication in the nose can distribute some of this medication to the Eustachian tube opening, allowing the inflammation and therefore the swelling to reduce. A nasal steroid spray does not get into the bloodstream and therefore does not expose the rest of the body to steroids. Topical steroid sprays take a week or two of daily use to achieve effect, are generally not as powerful as some of the other options listed, but can compliment them and are generally safe for long-term use when used properly.
Use of systemic (whole body) steroids. Steroids taken in pill or I.V. form do travel through the whole body via the bloodstream. This may be advantageous when the intended target(s) of the steroid cannot be reached otherwise, but the risks of side effects of steroids is a consideration. The risk of steroid use generally correlates to the dose and the duration of the steroid, thus a modest dose given for short duration is often best.
Avoid other irritants, including all forms of smoke.
tympanostomy tubes (aka pneumatic equalization tubes)
If more conservative management fails, creating a hole in the eardrum through a surgical procedure called myringotomy, essentially allows fluid or liquid to pass to and from the middle ear via the ear canal, thus bypassing the Eustachian tube. Myringotomy is usually accompanied by the insertion of a small tube that acts as a grommet to hold the hole open so that it does not heal closed after just a few days. This simple, low-risk and generally very effective technique helps relieve Eustachian tube dysfunction not only by bypassing the Eustachian tube with an alternate vent for air or fluid, but also by opening access for antibiotic ear drops placed in the ear canal to reach the middle ear, which would otherwise be blocked by the intact eardrum.
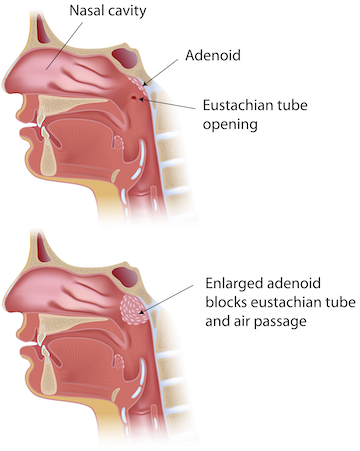
Removal of the adenoids (adenoidectomy)
Adenoids, which are located immediately adjacent to the Eustachian tube openings, are prone to infection, and this can worsen Eustachian tube function. Therefore, adenoid infection may be treated with antibiotics or removal of the adenoids (adenoidectomy). Surgical risk and recovery weigh against the advantage of adenoidectomy, relegating this procedure to a secondary effort after tympanostomy tube placement has already been performed. In other words, kids with significant Eustachian tube dysfunction typically get tympanostomy tubes as a first measure, and if and when a second set of tympanostomy tubes is needed, then adenoidectomy is usually included in with the procedure. Children over the age of four with chronic fluid behind the eardrum (chronic serous otitis media) typically have a recommendation for both tympanostomy tube placement and adenoidectomy.
Balloon dilation of the Eustachian tube
Another and more recent surgical technique to treat chronic Eustachian tube dysfunction is using balloon dilation of the Eustachian tube. Enlarging the lumen of the Eustachian tube is accomplished by briefly expanding a balloon catheter to stretch the Eustachian tube more open.
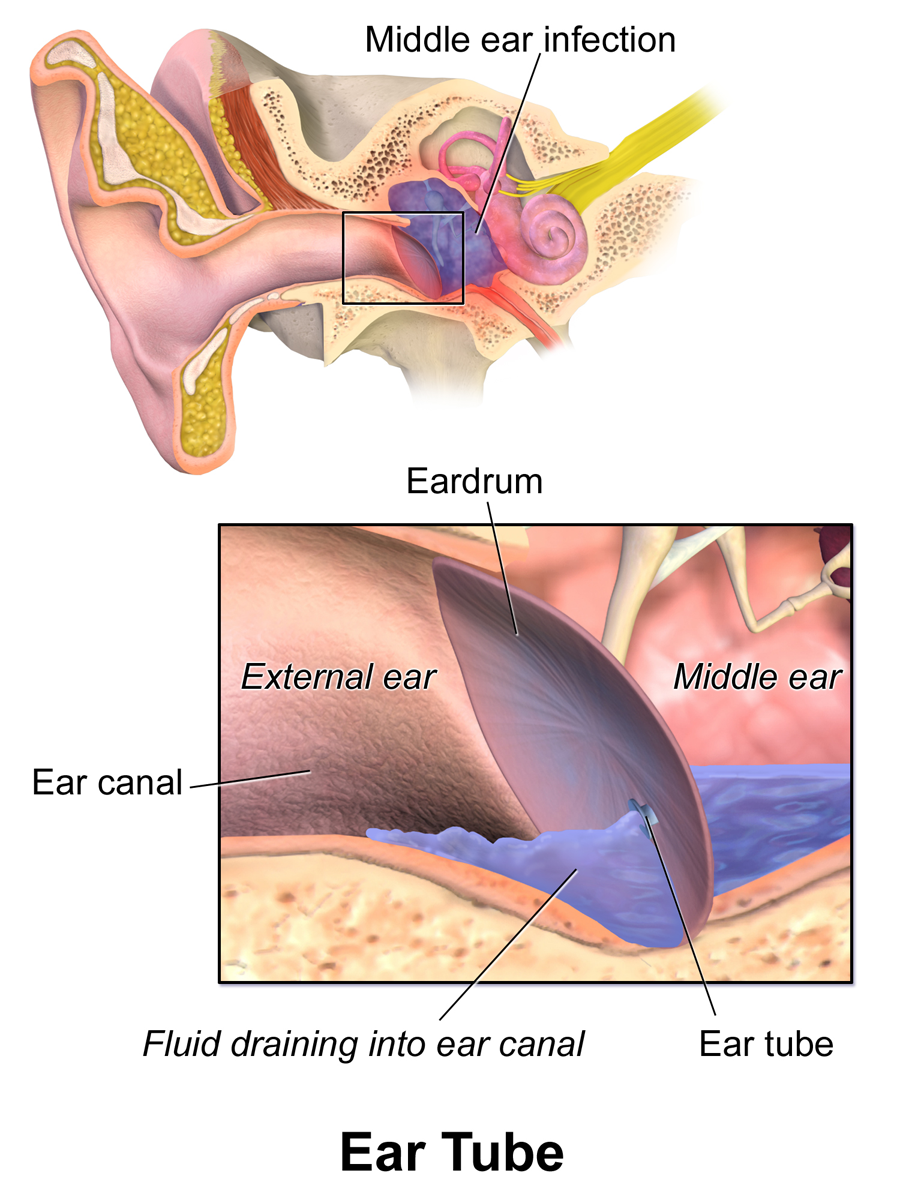
more on ear tubes (“PE” or Pneumatic equalization tubes)
Simple and very effective, an ear tube (also called pneumatic equalization tube, or ear ventilation tube) may be placed in a matter of minutes and work by doing the following:

Representation of a tympanostomy tube (shown in green), allowing air or fluid to pass through the opening (yellow arrow).
Allow air pressure to equalize on each side of the ear drum (not dependent on the Eustachian tube)
Allow fluid of pus from the middle ear space to drain out (which avoids the painful buildup of pressure and also makes home diagnosis of an ear infection accurate).
Allow antibiotic drops to get into the middle ear space
Technically, a small incision is made in the ear drum first, and the tube is placed in this hole to work as a grommet to keep the small hole from healing sooner than desired.
The tube usually stays in place for 1-2 years, although sometimes the body extrudes them sooner and other times or the tube may be retained in the tympanic membrane much longer. If no longer needed, the tube may be removed and the hole remaining may heal closed or be patched.
Generally, most adults can have tubes placed in the office without any sedation; kids have tubes placed in the operating room.

This page